Discussion»Questions»Health and Wellness» If I were to feel around on your body in non-sexual areas only, pick the major spot you would like worked in a massage?
The very good news is? You can do a lot yourself. That is a very reachable spot. And while it is great to just let go and let someone else do the massage, you can sit in a nice hot bath and do a lot of good to those tootsies.
Just start working them with your hands and do what feels right. Stretch the bones and take one side of foot and rotate it against the opposite side. Pull the toes gently. And make sure to use some lotion afterwards.
It will feel a lot better after this workout.
But you are right. Caching$$$$ feet are money to me. A lot of therapists don't like feet. I think feet make people want to return again and again.
Use a hot towel first and let the feet relax and then go to town.
Okay. Lie down crosswise on the bed. Have your trunk half-way off the bed and be lying on your back and just let the muscles relax for a good 5 minutes or however long it feels comfortable.
That is a tremendous stretch and will provide much relief if you can maneuver that position.
It's funny you should mention that. I just got hired at spa and for a tutorial I had to watch a video talking about boners and how to handle those who display one.
I have never had anyone get a boner yet. Maybe that is an insult to me. I want to stay insulted. I mean, there is no way to handle that. It is like farting. What do you SAY?
Ooops. Can you kindly put that away, sir? Or how about if I ice it and make it go down?
Okay. Lie down crosswise on the bed. Have your trunk half-way off the bed and be lying on your back and just let the muscles relax for a good 5 minutes or however long it feels comfortable.
That is a tremendous stretch and will provide much relief if you can maneuver that position.
I would start with nice cranial sacral massage. I think you might like that.
Craniosacral therapy (CST) is a form of bodywork or alternative therapy using gentle touch to manipulate the synarthrodial joints of the cranium. A practitioner of cranial-sacral therapy may also apply light touches to a patient's spine and pelvis. Practitioners believe that this manipulation regulates the flow of cerebrospinal fluid and aids in "primary respiration".[2] Craniosacral therapy was developed by John Upledger, D.O. in the 1970s, as an offshoot of osteopathy in the cranial field, or cranial osteopathy, which was developed in the 1930s by William Garner Sutherland.[2][3]
Although CST may relieve the symptoms of stress or tension, "available scientific evidence does not support claims that craniosacral therapy helps in treating cancer or any other disease".
Etymology
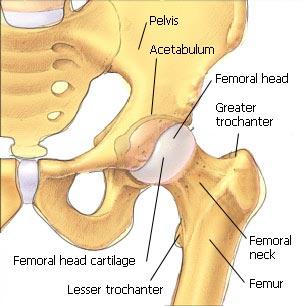
The term craniosacral or cranial-sacral are based on the terms cranium and sacrum, a bone of the pelvis which connects the lowest lumbar vertebra to the two hip bones and the tailbone. History and conceptual basis
Cranial osteopathy, a forerunner of CST, was originated by osteopath William Sutherland (1873–1954) in 1898–1900. While looking at a disarticulated skull, Sutherland was struck by the idea that the cranial sutures of the temporal bones where they meet the parietal bones were "beveled, like the gills of a fish, indicating articular mobility for a respiratory mechanism."
John Upledger devised CST. Comparing it to cranial osteopathy he wrote: "Dr. Sutherland's discovery regarding the flexibility of skull sutures led to the early research behind CranioSacral Therapy – and both approaches affect the cranium, sacrum and coccyx – the similarities end there."[8] However, modern day cranial osteopaths largely consider the two practices to be the same, but that cranial osteopathy has "been taught to non-osteopaths under the name CranialSacro therapy."
From 1975 to 1983, Upledger and neurophysiologist and histologist Ernest W. Retzlaff worked at Michigan State University as clinical researchers and professors. They assembled a research team to investigate the purported pulse and further study Sutherland's theory of cranial bone movement. Upledger and Retzlaff went on to publish their results, which they interpreted as support for both the concept of cranial bone movement, and the concept of a cranial rhythm. Later reviews of these studies have concluded that their research did not meet enduring standards to offer conclusive proof for the effectiveness of craniosacral therapy and the existence of cranial bone movement.
Practitioners of both cranial osteopathy and craniosacral therapy assert that there are small, rhythmic motions of the cranial bones attributed to cerebrospinal fluid pressure or arterial pressure. The premise of CST is that palpation of the cranium can be used to detect this rhythmic movement of the cranial bones and selective pressures may be used to manipulate the cranial bones to achieve a therapeutic result. However, the degree of mobility and compliance of the cranial bones is considered controversial and is a critically important concept in craniosacral therapy.[14] Primary respiratory mechanism
The Primary Respiratory Mechanism (PRM), the mechanism originally proposed by Sutherland, has been summarized in five ideas:
Inherent motility of the central nervous system Fluctuation of the cerebrospinal fluid Mobility of the intracranial and intraspinal dural membranes Mobility of the cranial bones Involuntary motion of the sacrum between the ilia
Inherent motility of the central nervous system
The postulated intracranial fluid fluctuation is described by practitioners as an interaction between four main components: arterial blood, capillary blood (brain volume), venous blood and cerebrospinal fluid (CSF). Fluctuation of the cerebrospinal fluid
There is research which demonstrates examiners are unable to measure craniosacral motion reliably, as indicated by a lack of inter-rater agreement among examiners. The authors of this research conclude this "measurement error may be sufficiently large to render many clinical decisions potentially erroneous". Alternative medicine practitioners have interpreted this result as a product of entrainment between patient and practitioner, a principle which lacks scientific support. Whether craniosacral motion can be reliably palpated remains a subject of debate with studies producing mixed results. Mobility of the intracranial and intraspinal dural membranes
In 1970, Upledger observed during a surgical procedure on the neck what he described as a slow pulsating movement within the spinal meninges. He attempted to hold the membrane still and found that he could not due to the strength of the action behind the movement. Mobility of the cranial bones
The extent to which cranial bones are able to move is considered controversial and studies of the existence and degree of cranial motion have yielded mixed findings. Cranial sutures are the areas in which the eight cranial bones are joined. During infancy, the cranial bones are not rigidly fused to each other, but are instead bound together by a membrane known as a fontanelle where two sutures join. Between the first and second year of life, the cranial bones begin to move together and fuse as a normal part of development. Studies examining the age of the closure of the cranial sutures have reported mixed findings. Closure has been reported to occur during adolescence while other studies indicate greater individual variability in the timing of this closure with fusion of the lambdoid suture, sagittal suture, and coronal sutures taking place in the fourth decade of life, but complete fusion of all sutures not occurring until advanced age (the eighth decade of life has been reported); some studies have found that the sutures never rigidly fuse. According to Gray's Anatomy, "[w]hen such sutures are tied by sutural ligament and periosteum, almost complete immobility results".
Treatment The therapist lightly palpates the patient's body, and focuses intently on the communicated movements. A practitioner's feeling of being in tune with a patient is described as entrainment.[18] Patients often report feelings of deep relaxation during and after the treatment session, and may feel light-headed. While sometimes thought to be caused by an increase in endorphins, research shows the effects may actually be brought about by the endocannabinoid system.
There are few reports of adverse events from CST treatment. In one study of craniosacral manipulation in patients with traumatic brain syndrome, the incidence of adverse effects from treatment was 5%. Reception







 This post was edited by WM BARR . =ABSOLUTE TRASH at July 19, 2017 5:54 PM MDT
This post was edited by WM BARR . =ABSOLUTE TRASH at July 19, 2017 5:54 PM MDT










 Bozette
Bozette